What is
Neurodivergence?
Neurodivergence refers to natural variations in how human brains are wired. Just as biodiversity describes the variety of life on Earth, neurodiversity recognises that there is no single 'right' way to think, learn or process information.
Neurodivergences are not mental health disorders, they are differences in brain development and function - often lifelong, often genetic - that affect how a person experiences and interacts with the world. This can bring both challenges and unique strengths.
Common Neurodivergent Terms
You Should Know
Neurodivergent vs Neurotypical
- Neurodivergent: A term used to describe individuals whose neurological development and functioning are atypical. This includes autism, ADHD, dyslexia, dyspraxia and other conditions.
- Neurotypical: A term used to describe individuals whose neurological development and functioning are considered 'typical' or 'standard.' It is a helpful term for distinguishing those without a neurological condition.
Diagnoses Commonly Included
Under Neurodivergence
The NHS and medical literature recognise the following as neurodevelopmental conditions, many of which overlap or co-occur.
ADHD (Attention Deficit Hyperactivity Disorder)
A neurodevelopmental condition involving inattention, hyperactivity and/or impulsivity.
→ ADHD overview
Autism
A developmental condition affecting how people communicate, interact and perceive the world.
→ Autism overview
→ Autism overview
Dyscalculia
A specific learning difficulty with understanding numbers and maths.
→ Dyscalculia overview
Dysgraphia
Affects handwriting and written expression.
→ Dysgraphia overview
Dyslexia
Affects skills involved in accurate and fluent reading and spelling.
→ Dyslexia overview
Dyspraxia (Developmental Coordination Disorder)
A condition affecting physical coordination, organisation and planning.
→ Dyspraxia overview
→ Dyspraxia overview
Pathological Demand Avoidance (PDA)
A profile currently understood to be on the autism spectrum characterised by high anxiety around everyday demands and a need for control.
→ Pathological Demand Avoidance overview
Tourette’s Syndrome
A neurological condition causing tics - involuntary movements or sounds.
→ Tourette's Syndrome Overview
The following conditions may be classed as mental health disorders.
Commonly Co-Occurring
Conditions
These conditions are not always formally diagnosed, but are commonly recognised in the community due to neurological differences or high rates of co-occurrence.
These may be part of someone’s diagnosis or exist alongside conditions like autism or ADHD. Many neurodivergent people identify with this umbrella based on lived experience and overlapping traits.
It is also important to acknowledge that neurodivergence can occur without learning difficulties - those without learning difficulties are often high masking, and my not immediately exhibit stereotypically obvious signs of neurodivergence.
Auditory Processing Disorder (APD)
Difficulty interpreting sound, even with normal hearing.
→ APD overview
Developmental Language Disorder (DLD)
Persistent difficulties in understanding or using spoken language.
→ DLD overview
Hyperlexia
Early and advanced reading ability, often paired with comprehension or communication challenges.
→ Hyperlexia overview
→ Hyperlexia overview
Nonverbal Learning Disorder (NVLD)
Strong verbal skills combined with challenges in spatial awareness, motor skills and social interaction.
→ Nonverbal Learning Disorder overview
Sensory Processing Disorder (SPD)
Difficulty processing sensory information. Common in autistic and ADHD individuals.
→ Sensory Processing Disorder overview
Synaesthesia
A cross-wiring of the senses e.g. 'tasting' colours or 'seeing' sounds.
→ Synaesthesia overview
Medical vs. Social
Models of Disability
There are two main frameworks for understanding neurodivergence:
- Medical Model: Focuses on diagnosis and deficits
- Social Model: Focuses on barriers
Using the social model is a great way to ensure inclusion and accessibility enabling all cast and crew to thrive. The industry is simply not yet built to help neurodivergent people thrive. However, many steps are being made in the right direction so that one day, we will be able to create a workplace where all neurotypes can create their best work.
The TAP toolkit provides further information on the social model of diasbility.
The Non-Linear
Nature of the Spectrum
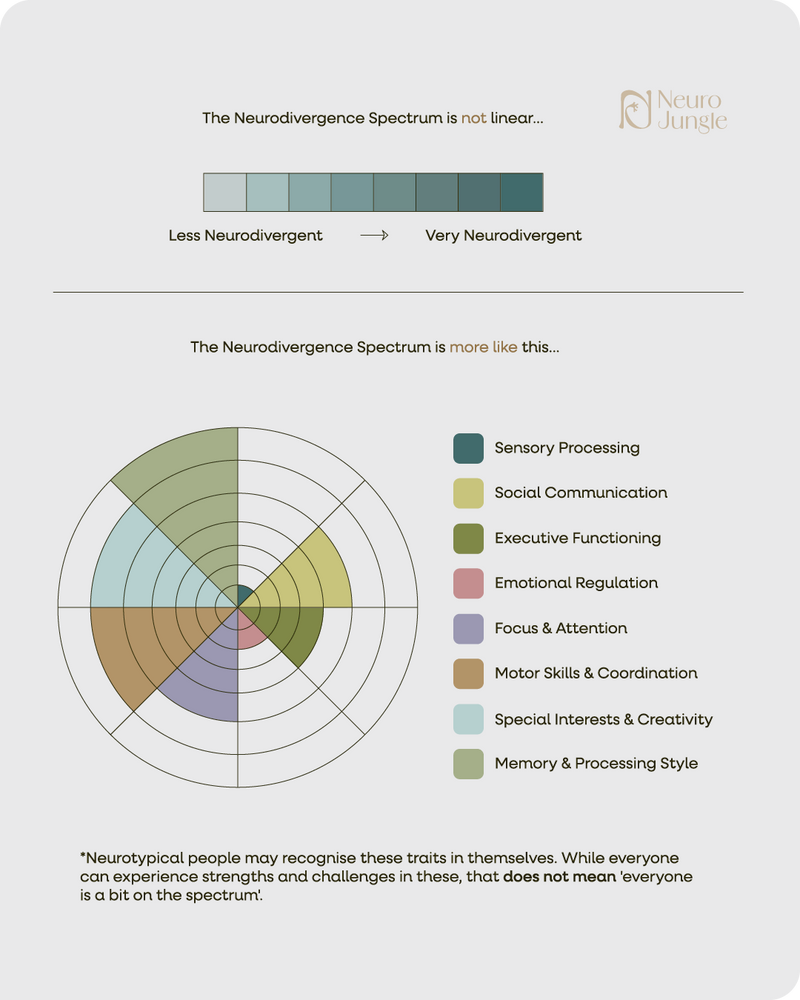
The 'spectrum' is not a line from 'more' to 'less' autistic or ADHD - it is a spiky profile: people have higher and lower support needs in a range of different areas and these needs can fluctuate over time or in different environments.
Physiological &
Genetic Foundations
Neurodivergence is a measurable, neurological difference that comes from a person’s genetics and is passed down through families.
Below are some examples of the physiological differences that can be seen:
Autism
-
Less synaptic 'pruning' in adolescence leads to increased neurone connectivity in the brain’s cortex. This leads to heightened sensitivity to sounds, lights, movement, textures and can cause overwhelm.
-
Enlarged amygdala: the amygdala is responsible for the fight/flight/freeze/fawn/flock response to threats, which can include a racing heart, sweating and a feeling of panic. The larger amygdala in autistic people causes a much larger response, which can be perceived as an 'over reaction.' It is important to remember that this is a physical response caused by the brain’s perception of a threatening environment, which cannot be controlled by the autistic person.
ADHD
-
Dopamine is absorbed more quickly in the brain, meaning that the feeling of reward after completing a task is much shorter.
-
ADHD medication works by slowing that absorption, allowing dopamine to stay available for longer and creating a bigger feeling of reward after task completion.
-
Smaller basal ganglia, which is linked to motivation, task initiation and goal-setting.